Banner

Title
Five Things to Know About Autism in Minnesota
Body
This fall as they headed back to school, many of our state’s kindergarteners have just been screened for the first time to identify potential health or developmental problems. For many families, they’ve learned (or received confirmation of concerns they already had) that their child is exhibiting symptoms of autism spectrum disorder, or ASD.
This can be a stressful time for families as they begin the process of understanding what it means for a child to have ASD and how it will impact their child’s and family’s lives, as well as what resources are available for them. Teachers and others who work with children also need to learn more about and use available resources to support them in finding the best ways to work with children on the autism spectrum.
Wilder Research has been working with the Minnesota Department of Human Services to evaluate the Early Intensive Developmental and Behavioral Intervention (EIDBI) benefit, which serves children with autism. Through this process, we’ve taken a look at the prevalence of autism in Minnesota.
Here are five things to know about autism in Minnesota:
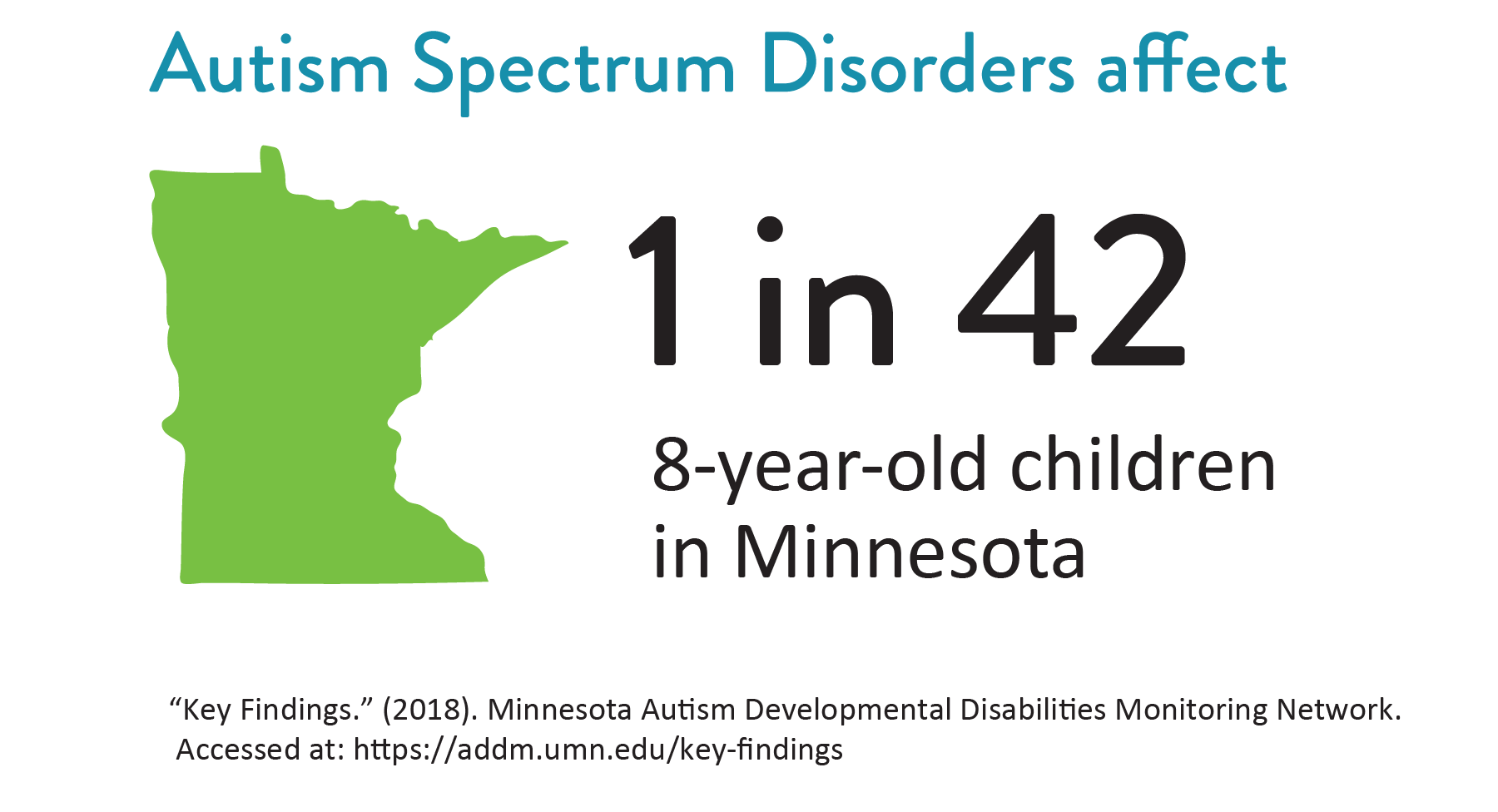
1. Autism spectrum disorders affect 1 in 42 Minnesota children.
This is higher than the national average of 1 in 59. This could be due to a number of factors, but it’s likely that we in Minnesota are just diagnosing children with autism at higher rates, rather than Minnesota children having a higher prevalence of autism than other states. (Prevalence rates are based on best available data, which is largely focused in metropolitan areas.) Right now, we don’t see any significant differences in autism prevalence by race or ethnicity.
2. Autism is being diagnosed in children later than is ideal.
Children can be diagnosed as early as 18 months old, but the average age of diagnosis in Minnesota is 4 years and 9 months (about the time that youth go through pre-kindergarten screening). Parents and those who regularly work with young children should pay attention to potential signs of autism and work with their child’s pediatrician as well as other experts to ensure a medical diagnosis and educational determination can be made as soon as possible. This will lead to earlier intervention, which we know is a key factor in determining the child’s long-term outcomes.
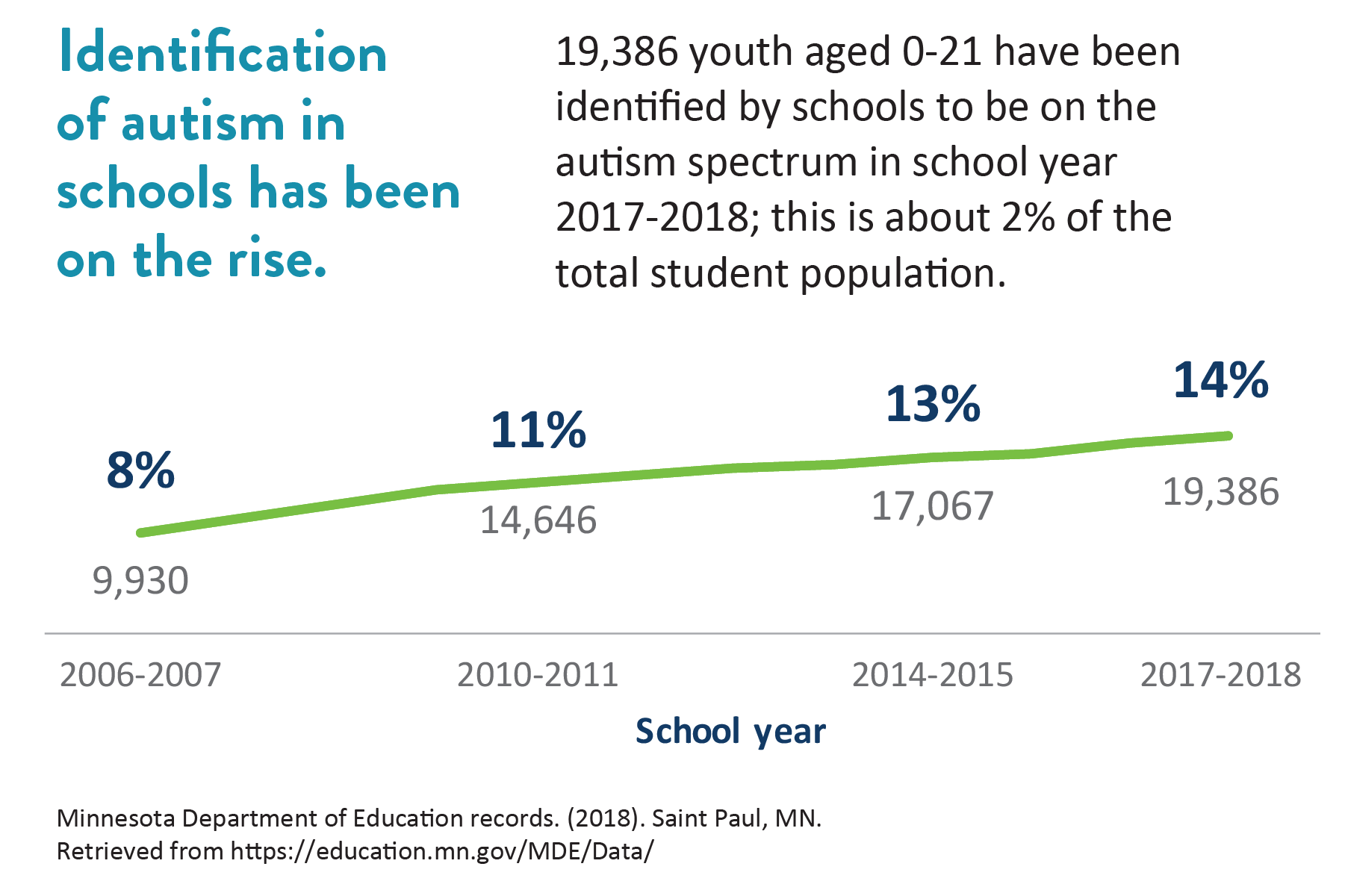
3. Identification of autism in schools has been on the rise.
Educational determination is different from a medical diagnosis. While 19,386 youth have been identified within Minnesota’s school systems to have autism as of the 2017-18 school year, less than half of those (8,878 youth) have a clinical diagnosis of autism. To be eligible for many state and county services, children need to have a clinical diagnosis of autism spectrum disorder and not just an educational determination.
4. Children with autism can receive school-based services even before they enter school.
There are a variety of resources available to young children and their families, even before they formally enroll in kindergarten. Parents should reach out to their school district to see what their local schools can provide for their child in terms of Part B and Part C Early Childhood Family and Special Education services.
5. Children with autism and related conditions and their families can face a variety of barriers to being diagnosed and receiving appropriate care.
Cultural differences and language barriers can keep professionals from noticing warning signs and delay diagnosing children from different cultural backgrounds and those who do not speak English at home. Additionally, many diagnostic tools were developed in European countries and are not tailored to meet the needs of cultural communities with varying ideas about how people are expected to socialize with one another. For example, limited eye contact is commonly considered to be a potential sign of autism, which reflects Western ideas about what the appropriate level of eye contact is. Health care providers, educators, and others working with children should be aware of cultural differences in awareness of and attitudes toward autism and related conditions as well as differences in how autism may present in children from different cultural backgrounds.
Conversations around autism are generally deficit-focused. While that’s essential to receive a medical diagnosis, educational determination of autism, and accessing related services, it’s important to remember that children (and adults) with autism bring a wealth of skills, perspectives, and personality traits that make the world a better place. Those working with and for individuals on the autism spectrum should aim to appreciate those differences by using a strengths-based and person-centered approach.
Read more about what we learned
Widgets
- Minnesota Autism Resource Portal
- ASD Strategies in Action
- Child and Teen Check-ups Fact Sheet
- EIDBI 101 trainings for parents and providers
- Help Me Grow Minnesota
- Minnesota Department of Human Services person-centered training opportunities
- For general information and responses to questions and comments from the Minnesota Department of Human Services, email ASD.DHS@state.mn.us